Carpal tunnel syndrome, Geelong
What is the carpal tunnel?
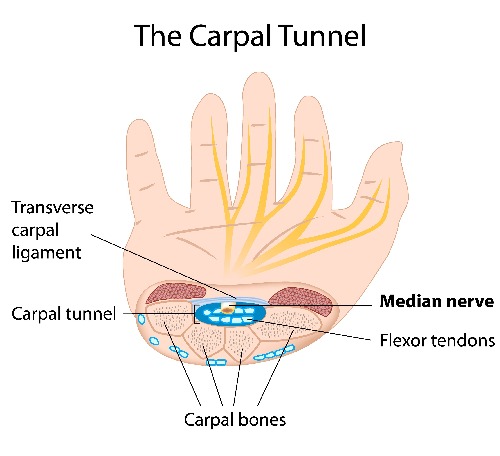
The carpal tunnel is a space at the level of the wrist bound by the bones of the wrist (carpal bones) at the back and a strong fibrous band at the front, called the transverse carpal ligament. One of the main nerves to the hand, the median nerve, travels through this tunnel along with tendons to the fingers. The median nerve provides sensation (feeling) particularly to the thumb, index, middle and ring fingers, as well as supplying some of the muscles around the thumb.
Who gets carpal tunnel syndrome?
- More common in women than men
- Fifty percent of patients are between 40 and 60 years of age
- Approximately one to two percent of people may develop carpal tunnel syndrome during their lifetime.
What causes carpal tunnel syndrome?
- In most patients there is no known cause.
- Medical conditions such as diabetes and hypothyroidism.
- Arthritis in the joints around the wrist.
- Pregnancy.
- Work is unlikely to be a significant contributor, except possibly heavy repetitive work performed in cold conditions.
What are the symptoms?
- Burning or aching pain in the hand(s), possibly extending up into the arm.
- Pins and needles especially in one or more of the thumb, index, middle and ring fingers. Rarely does this occur in the little finger.
- Symptoms commonly occur at night, when driving, when using a firm grasp or when the wrist is bent forwards or backwards.
- Tendency to drop objects.
- Difficulty with tasks requiring fine movements of the fingers.
Why does it happen?
- When the nerve becomes compressed within the tunnel, the blood supply to the nerve is interrupted, causing the symptoms to develop.
- The size of the tunnel is reduced when the wrist is bent forwards or back – this is why symptoms occur in these postures.
- Symptoms often occur at night because our blood pressure drops when we sleep and the wrist may fall into a bent position – all of these can affect the blood supply to the nerve.
- Symptoms may occur with a sustained grip such as holding a steering wheel, a telephone, or a book/newspaper.
Do tests need to be done?
- Nerve conduction studies performed by a neurologist (nerve specialist) are required to confirm carpal tunnel syndrome. Small electrodes are placed in the skin to measure sensation and muscle function.
What is the treatment?
- Splints: Splints to keep the wrist in a straight position may help the symptoms, though not cure the condition. These may be useful especially at night.
- Steroid injection: Injections into the carpal tunnel may help to settle the symptoms. The steroid may not start to work until one to two weeks after the injection. Some patients are completely cured, however a large number redevelop the symptoms after two to three months as the effects of the steroid wear off.
- Surgery: Carpal tunnel release aims at dividing the transverse carpal ligament to create more space in the tunnel (see below).
What will happen if there is no treatment?
- It is unpredictable what will happen in each individual case.
- If the nerve is compressed for too long the nerve may be damaged, potentially resulting in permanent loss of sensation and/or strength.
Surgery for carpal tunnel syndrome
- Hospital stay: Usually day case. Alternatively the procedure may be performed in the rooms.
- Anaesthetic: Commonly under local anaesthetic with or without sedation. Surgery may also be performed under regional (arm block) or general anaesthesia. This may be discussed with the anaesthetist. If performed in the rooms, this is done under local anaesthetic only.
- The procedure: A tourniquet is placed on the arm to control bleeding. A small cut (approximately five cm) is made in the skin at the wrist. The transverse carpal ligament is divided. The nerve is inspected though usually not disturbed. Approximately three stitches are placed in the wound and a firm supportive bandage is then placed on the wrist, allowing the fingers and thumb to move freely. The operation may also be performed endoscopically via two small cuts. The recovery from surgery using this method is faster though there is a slightly higher risk of nerve injury.
- Complications: These are unusual. Overall, this is a very successful procedure and the vast majority of patients obtain relief of their symptoms. However, with any surgical procedure there are risks involved. These will be discussed at length at your consultation with Mr McDonald.
After the operation
- Keep the hand elevated above the level of your heart to minimise swelling and bleeding. A sling will help you keep the hand in the correct position. Rest it on pillows at night
- Keep your fingers and thumb moving. You still may use the hand to hold a toothbrush, knife or fork, though nothing much more than this.
- Keep the bandages dry. Tape a plastic bag over your hand and arm when showering, keeping the hand elevated.
- An appointment will be made for you to return to have the bandages removed and the wound checked five to six days after the operation. At that stage a small piece of dressing tape will be used to cover the wound. This may get wet in the shower. Allow the tape to air dry, or dry it with a hair dryer following your shower.
- Dissolving sutures are used, over the following 10 to 14 days the sutures will fall/pull out.
- Hand therapy – in a small number of patients who experience prolonged swelling and stiffness, hand therapy may be valuable in helping the hand regain full function.
Resuming activities
- No heavy lifting (nothing more than one kilogram) or repetitive tasks are advisable for at least six weeks after operation. Light tasks may be resumed earlier. Patients are encouraged to work on their grip strength with a squeeze ball from six weeks onwards. Some patients notice strength in the hand is reduced following surgery.
- There can be some discomfort around the scar as you increase your activities. Sometimes this discomfort can last up to six months. It usually relates to the scar maturing. Massaging the scar may help.
- Once stitches have come out it may be possible to resume driving a car, though it is advisable to take short drives initially. If a lack of movement or discomfort impedes your ability to drive, then you should allow more time for your hand to settle.
Recurrence of carpal tunnel syndrome
- This is unusual. Sometimes many years after surgery, often in the setting of arthritis or the development of certain medical conditions, the symptoms can return.
Do you suffer from Carpal Tunnel Syndrome? Consider making an appointment with Geelong plastic surgeon, Mr Anthony McDonald. Mr McDonald will assess your condition and determine the best treatment plan for you. Contact Anthony McDonald Plastic Surgeon on (03) 5221 7002 for this or any other condition of the hand that is causing you pain or discomfort, such as arthritis, ganglions and trigger finger.